VERTIGO
Definition: Vertigo refers to a specific symptom describing a false sense of motion, usually spinning or rotatory, in the surroundings or within oneself despite the absence of physical movement. In clinical practice, the term ‘vertigo’ is not usually volunteered by patients.
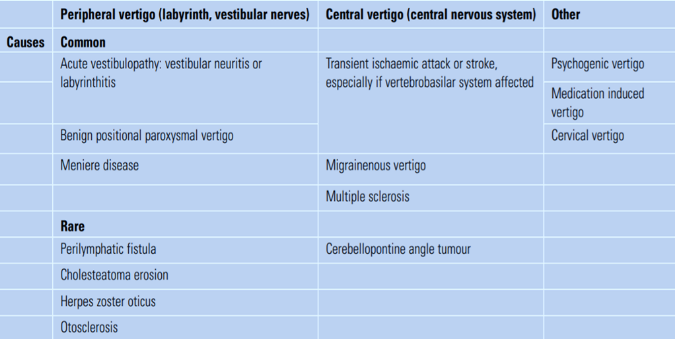
Causes
The labyrinth is an inner ear neurosensory organ made up of two components – Semicircular canals (for balance) and Cochlear (for hearing). Typically, vertigo is caused by an imbalance of sensory inputs into the two vestibular nuclei from over activity or underactivity of either or both sides of the labyrinth. The brain interprets such input differences as a sensation of movement. However, any disturbances to the labyrinth, visual-vestibular interaction centers in the brain stem and cerebellum, and sensory pathways to or from the thalamus, can result in vertigo. Causes of vertigo are divided into central or peripheral origins:
- Benign paroxysmal positional vertigo (BPPV)
- Acute peripheral vestibulopathy (vestibular neuritis or labyrinthitis)
- Meniere disease
Central causes of vertigo, although not as common, are generally more serious and should always be considered.
Clinical assessment
The clinical assessment is aimed at determining if the patient has true vertigo, whether the vertigo is of central or peripheral origin, and to rule out life threatening conditions such as cerebellar hemorrhage.
1. History Taking
2. Examination-
- General inspection looking for patterns of facial asymmetry suggesting either peripheral facial nerve involvement or a cerebrovascular event
- Visible vesicles of herpes zoster on the external ear
- Otoscopic examination revealing signs of inflammation associated with acute vestibulopathy, scarring of the eardrum from chronic suppurative otitis media, or an erosive cholesteatoma
- Positive Hennebert sign when vertigo is reproduced by applying external pressure on the tragus, suggesting the presence of a perilymphatic fistula
- Observation for features of nystagmus such as spontaneity, direction, and associated changes with eye movements, conveying valuable diagnostic information
- Horizontal and torsional nystagmus, which beats to a unilateral direction regardless of whether the eyes are gazing to the left or right, suggesting peripheral origin of vertigo
- Direction of nystagmus changes when the eyes are gazing toward a different direction, indicating a central cause of vertigo
- Vertical nystagmus implying central and brainstem involvement
3.Clinical tests-
- The head impulse test is both sensitive and specific to detect unilateral hypofunction of the peripheral vestibular system, which is commonly due to acute vestibulopathy
- A functional vestibular system can detect small changes in head position and rapidly adjust eye movements to keep the center of vision on a target
- In patients with acute vestibulopathy, when the head is turned toward the affected side, there will be a delay in vestibular adjustment, manifesting as a brief and fixed gaze toward the affected side followed by a corrective saccadic eye movement back to the center
- The head impulse test is important in differentiating between cerebellar infarction and acute vestibular neuritis
- If the head impulse test is normal in patients with acute vertigo, acute vestibulopathy is ruled out and cerebrovascular causes of vertigo, such as ischaemia or infarction, should be considered
1. The Romberg test
2. The Fukuda-Unterberger test–
3. The Dix-Hallpike manoeuvre-
Management of an acute vertigo attack
- An acute and severe episode of vertigo, regardless of the underlying cause, will usually settle by itself within 24-48 hours due to the effect of brainstem compensation
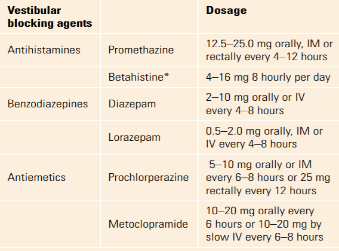
- During the acute phase, supportive measures, bed rest, anti-emetics, and vestibular blocking agents can be used to provide symptomatic relief
- Betahistine is known to selectively increase blood flow to the inner ear
- A combination of an antihistamine (e.g., promethazine) and an antiemetic is commonly used
- The use of vestibular blocking agents can delay the compensatory mechanism of the brainstem and prolong the symptoms of vertigo, and may carry risks of side effects
- Therefore, prolonged use of symptomatic medications for acute vertigo is best avoided, especially if a specific treatable cause is identified
Management of vertigo with specific causes
Benign paroxysmal positional vertigo
- Benign paroxysmal positional vertigo (BPPV) is the most common underlying cause of vertigo.
- The pathophysiology of BPPV is the lodgement of a 'canalith' inside the posterior semicircular canal.
- A canalith is made up of small crystals of calcium carbonate that have detached from the utricle in the vestibule of the inner ear.
- Movement of the canalith activates vestibular hair cells to create an overall asymmetrical vestibular input.
- Patients usually experience a brief but intense vertigo when they turn in bed at night or change their head position.
- The most important clinical test to perform is the Dix-Hallpike manoeuvre.
- A positive Dix-Hallpike manoeuvre serves three purposes: to confirm the diagnosis, to localize the affected side, and to demonstrate canalith mobility.
- The Epley or canalith repositioning manoeuvre (Brandt-Daroff exercises or the Semont manoeuvre) is a safe and effective way to treat BPPV.
Acute peripheral vestibulopathy
- Vestibular neuritis describes an inflammation of the vestibular nerve which results in severe vertigo that usually lasts for days.
- Labyrinthitis is similar to vestibular neuritis but also includes hearing loss as an additional feature.
- Viruses such as mumps and influenza are thought to be the causative organisms.
- Cerebellar infarction is a major differential diagnosis and should always be considered.
- During the acute phase, patients benefit from bed rest and short-term symptom relief treatments.
- A high dose of prednisolone (125 mg) is given and the dosage is slowly tapered down over 18 days.
- Antiviral medication has not been shown to be of any benefit.
- In patients with suppurative labyrinthitis, usually following a bacterial otitis media infection, hospitalization with intravenous antibiotic treatment is required.
- Early mobilization as tolerated in a safe environment will encourage the brainstem compensatory mechanism.
- Vestibular rehabilitation exercises can also be introduced to allow a more rapid and complete compensation of vestibular function.
Meniere disease
- Meniere disease is caused by an idiopathic abnormal dilatation of endolymphatic organ producing symptoms of progressive vertigo, tinnitus, aural fullness, and fluctuating low-frequency hearing loss.
- There is no cure for Meniere disease, so treatment is focused on relieving the debilitating vertigo.
- Acute treatment of an attack may include bed rest, antiemetic, and vestibular blocking agents.
- A low salt diet (<1-2 gm/day), diuretics, and betahistine are recommended treatments.
- In patients with severe debilitating vertigo, labyrinth ablation therapies with intratympanic gentamicin injection or surgical repair or removal of the labyrinth may be required if conservative and medical treatments have failed.
- Unfortunately, there is currently no effective treatment for hearing loss and tinnitus in Meniere disease.
- Regular clinical assessments and formal hearing tests are important to monitor disease progression.
Trauma induced vertigo
- About 80% of patients experience vertigo following head trauma, and 20% of these patients continue to have residual vertigo at 6 months.
- Head trauma can either cause direct injury to the labyrinth and its central connections or can cause a canalith dislodgement resulting in a BPPV-like syndrome, which can be treated accordingly.
- Cervical vertigo, which occurs following a whiplash neck injury, is a specific syndrome of dizziness associated with neck pain. Treatment is done with physiotherapy and neck immobilization.
- A perilymphatic fistula, commonly due to barotrauma, is typically found in people who work in an environment with sudden atmospheric pressure changes, such as pilots or divers. The fistula will usually heal after 2 weeks from the onset of symptoms with appropriate bed rest and avoidance of straining and coughing.
- Initial and follow-up audiological assessments are mandatory, and surgical repair is required if there is progressive hearing loss.